At my son Qiqi’s six-month wellness checkup in April 2024, his pediatrician noticed head shape deformity and referred us to a clinic specializing in helmet therapy for babies in Austin, Texas. The pediatrician also suggested that we visit the helmet clinic soon because the effectiveness of helmets decreases after six months. I then took Qiqi to the helmet clinic for an evaluation. The clinic is part of a nationwide network of clinics operated by a leading helmet manufacturer. Helmet therapy for babies is its sole service and all on-site clinicians are licensed occupational therapists. One of the clinicians assessed Qiqi’s head shape issue to be on the border between mild and moderate, leaning towards moderate, and recommended he wear a corrective helmet.
Infants’ cranial deformities can be congenital or positional. The former, called craniosynostosis, refers to the premature fusion of babies’ cranial suture(s), which can cause irregular head shape and neurological damage. Craniosynostosis is a rare medical condition that requires surgical intervention and subsequent helmet therapy. In contrast, positional cranial deformity, also called plagiocephaly, is a cosmetic issue. Because babies’ skull bones are soft, consistently sleeping in the same position can result in a flat spot on their heads, which can make their heads asymmetrical. This doesn’t cause any pain or impact brain development. Plagiocephaly is common1 and can be ameliorated by changing babies’ lying positions, more tummy time, and physical exercises with neck muscles. In addition to these conservative methods, plagiocephaly can be treated with a corrective helmet to remold babies’ head shape.
Since Qiqi’s head shape issue was a cosmetic concern related to plagiocephaly, his pediatrician told us that it would be up to us as parents to decide whether to undertake helmet therapy. As I read the pamphlet that explained helmet therapy, I became troubled by the idea of a “normal” head shape. As an anthropologist, I wondered: how is the normal defined, and by whom? What kinds of head shapes, in terms of race and ethnicity, are modeled as normal? Why should head shapes look such a specific way (a specific proportion of cranial width to length; symmetrical on two sides; a curved back)? For the first time ever, I assessed my own head shape by hand and realized that it was asymmetrical. I also found the back of my partner’s head flat, which I had never noticed before. Unbeknownst to us, there was now a standard for head shape that required parents to seek medical assessment and intervention in their children’s early infancy.
As a mother, however, I cannot stop being anxious. The therapist at the helmet clinic emphasized a short treatment window because babies’ skulls harden rapidly. According to the therapist, babies between three and four months only need to wear helmets for five to seven weeks. The duration of treatment increases by the severity of the baby’s condition and their age. Qiqi would need to wear the helmet for three and a half to four months because of his age. We were running late. Such urgency amplified my anxiety with guilt and pressured me to start the therapy promptly. My friends whose children underwent the therapy told me that they were afraid to miss the narrow timeframe and were trying to avoid regrets in the future.
Helmet therapy was first adopted in 1979 by S.K. Clarren, D.W. Smith, and J.W. Hanson, a group of pediatricians in University of Washington School of Medicine. They created helmets themselves to treat ten infants with significant deformational plagiocephaly. It was not until 1998 that the FDA first approved a manufactured helmet to treat plagiocephaly. A study showed that, by 2013, there were thirty-seven cranial orthotic devices approved by FDA. In 2016, the Congress of Neurological Surgeons (CNS) released an evidence-based guideline that recommended helmet therapy for older infants with moderate to severe plagiocephaly when conservative methods proved ineffective. The guideline doesn’t specify a quantified treatment threshold, and the overall strength of the CNS guideline is level II, indicating “uncertain clinical certainty.”2
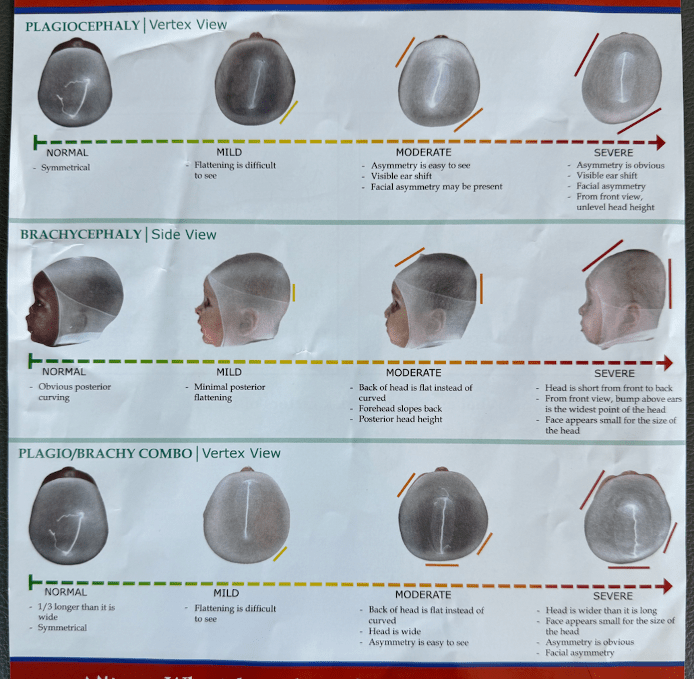
The helmet clinic provided an evaluation report containing two metrics to assess asymmetry for plagiocephaly and one metric measuring the proportion between cranial width and length. For each metric, a numerical indicator is assigned. These indicators are displayed on a gradient-colored bar ranging from green to red, illustrating the continuum from normal to severe. My son’s three indicators are placed at dark green, green, and a point where the green hue begins to fade. Although the numerical indicators are quantified and seemingly objective, it is unclear how these metrics are integrated to make diagnoses. My son’s cranial deformity was overall diagnosed as “moderate,” and the helmet therapy was recommended.
The estimated cost for the helmet therapy is $1,900. The severity of my son’s head shape situation doesn’t meet the requirement for insurance coverage. But a clinic staff member told me that, “although the insurance company doesn’t cover your case, it doesn’t mean the helmet isn’t necessary.” This seems to be another case in which biotech companies redefine the line between normal and abnormal to expand markets. Indeed, it is increasingly common to see babies wearing corrective helmets in different parts of the world.3 The uptake of the device reminds me of the story of dental orthodontics, which have become so normalized that perfectly aligned teeth have subtly become a marker of social status. It appears that social inequalities are becoming etched onto human bodies at young ages through head shape, teeth alignment, and whatever new normal that is emerging. Although I hate to give credence to the idea of “normal” head shape, for a time, I still hesitated. What if, in the future, Qiqi’s head shape would create boundaries between inclusion and exclusion. What if Qiqi would one day wish that he had worn a helmet?
Medical anthropologists have shown that the commodified, anticipatory pursuit of optimal health has become a virtue, especially among the middle-class. I find that anticipatory decision-making is also central to today’s middle-class ethics of parenting in the US. Health and behavior issues nowadays require early detection and intervention, and anticipatory parenting is closely intertwined with consumerism. On one hand, health and behavior issues extend beyond diseases to include everyday consumer decisions. In online forums, parents discuss materials and ingredients when purchasing everyday essentials like formula, formula bottles, toys, and baby food to prevent possible exposure to toxins. On the other hand, new medical demands are being created with sales incentives, of which helmet therapy may be an example. The helmet company’s promotional slogan is “Reshaping Children’s Lives.” The implication is that helmets are not just correcting babies’ head shapes in the present but have a long-term impact on their lives.
Further, anticipatory parenting is compatible with and fueled by neoliberalism. Anticipatory decision-making produces ceaseless anxieties. Whether a judgment is right or wrong will remain unknown for an extended period. These medical/consumerist decisions focus on atomized body parts and technical devices. Take the helmet therapy as an example: what kind of better future can a “normal” head shape provide? The direct answer is better and “normal” appearance. Hypothetically, improved appearances may boost confidence and facilitate social life. However, as a person of color and a child of first-generation immigrants, Qiqi has much bigger structural challenges—such as racism—to battle growing up. Compared with those structural problems, head shape deformity, if it is indeed a problem, seems to be insignificant.
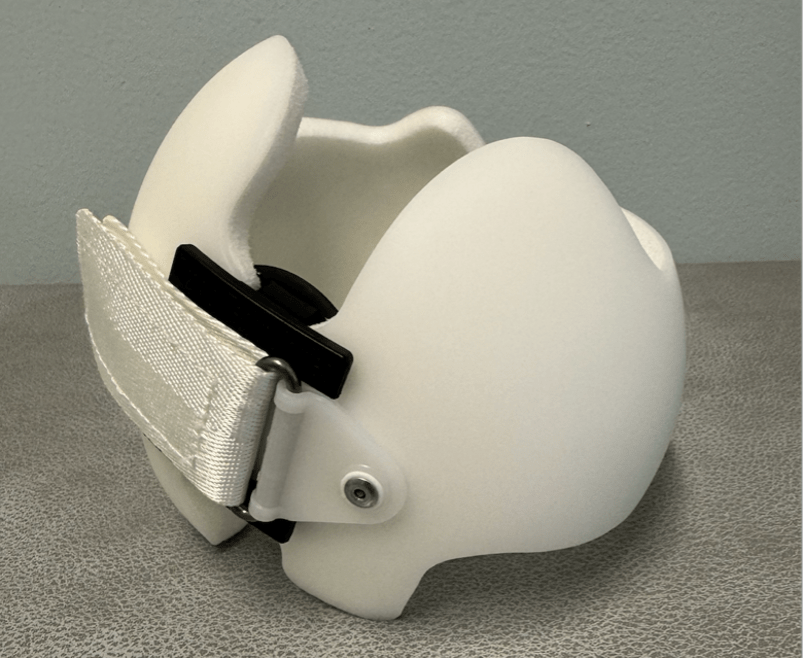
After serious consideration, I decided not to start the helmet therapy for my child. The anticipatory benefits of helmet therapy come at the expense of babies’ current comfort and well-being. The helmet needs to be worn twenty-three hours a day, which causes extreme heat and can easily trigger rashes and eczema. As my son’s skin is eczema-prone, wearing the helmet for almost four months in a Texas summer will be torturous. I cannot convince myself to subject him to physical discomfort to adhere to an aesthetic norm that I don’t believe in. In Qiqi’s evaluation report, the relatively “abnormal” metric is one called Cephalic Index (CI), which measures the proportion of cranial width and length. His CI indicates a condition called brachycephaly, referring to a head shape that is wider than ideal and flat on the back. I cannot understand why everyone’s head should have a curved back. And why should such specific aesthetic standards for head shape be so universal?
Interestingly, the concept of CI has a history in physical anthropology. From the eighteenth to early twentieth century, European physicians and anatomists used cranial measurements to differentiate between human races and apes. Polygeny, a prominent school of thought of that era, relied on skull sizes and shapes to categorize racial groups and to advocate for racial hierarchies. Samuel George Morton (1799–1851), a representative polygenist in the early eighteenth century, associated cranial size with intelligence. He adopted cranial size as a criterion to rank racial differences and placed “Caucasians” at the top of intelligence rankings. CI was devised during that era by Anders Retzius (1796–1860), a Swedish anatomist, polygenist, and anthropologist, to classify racial variances.
In 1912, Franz Boas published an article titled Changes in the Bodily Form of Descendants of Immigrants, which was a notable departure from the racist understanding of human differences. Boas disputed the idea of using CI as a biological trait to classify racial groups. Instead, Boas argued that head shape could be affected by environment and nutrition. Still, the racist utilization of head and facial measurements continued throughout the first half of the twentieth century, reaching its zenith in Nazi Germany, where such metrics were employed to identify Jews.
In the past, the CI was problematically adopted to understand human differences; now, corrective helmets are being used to normalize babies’ CI. That is to say, brachycephaly has shifted from being considered a mark of inherent inferiority to being pathologized. My son’s evaluation report listed two references for CI, both of which addressed “craniofacial anthropometry.” Craniofacial anthropometry is a field pioneered by Leslie Farkas, a Hungarian plastic surgeon, who moved to Prague after the World War II. Farkas collaborated with Karel Hajniš, a physical anthropologist at Charles University, and borrowed the method of anthropometry from physical anthropology to take facial measurements for the treatment of facial deformities. In modern biological anthropology, however, anthropometry is controversial and outdated because of its racist past.
Farkas moved to Toronto in 1968, where he continuously collected anthropometric data and developed quantified databases to measure the human face and head for planning and assessing plastic surgery. It was not until late in his career that Farkas started to include data from non-white populations.4 In his 1987 book Anthropometric Facial Proportions in Medicine, Farkas and Munros established the CI norm for children under one year old, based on data collected by the Czech anthropologist Karel Hajniš’. Hajniš gathered his data from a limited sample size of 134 infants in West Germany in 1974. Still, this CI metric became the norm and remained the standard for three decades. Since the American Academy of Pediatrics began advising that infants should sleep on their backs in 1992, the mean CI among American infants has been growing. Although there is medical literature that advocates redefining the current normative CI and called for attention to cultural impacts on CI, major insurance companies today still refer to the CI norm derived from Hajniš’s data to evaluate medical necessity. The helmet clinic’s therapeutic recommendation is stricter than the insurance companies.
Life is easier being normal. However, medicalized and commercialized norms such as CI perpetuate a white-centric legacy. As a parent, I often ask myself: how do I best support my child to negotiate such norms as a person of color growing up in America?
Acknowledgements
I thank Celina de Sá for suggesting this title and encouraging me to write this article. I am grateful to Ainash Childebayeva and Rebecca Lewis for providing invaluable insights and resources on physical anthropology. Many thanks to the editors Jessica Robbins-Panko and Alex Nading for their thoughtful feedback and insightful comments.
Notes
1. A 2010 epidemiological study conducted in Canada, involving 440 infants, shows that 46% of them in this study have a certain degree of plagiocephaly. The 46% incidence rate is widely cited.
2. This guideline is based on a systematic review of fifteen published studies about the efficacy of helmet therapy for plagiocephaly. This guideline acknowledged lack of data on long-term effect of helmet therapy and on the natural improvement of positional plagiocephaly. The cost of helmet therapy also compromises its recommendation level.
3. As far as I know, a US-based helmet company has opened clinics in major cities in China. The cost is around 28,000 yuan (~$4,000).
4. In a 2005 study, Farkas et al. took arthrometric data from people, in their own terms, from the Middle East, Asia, and of African origin.
Xisai Song is Assistant Professor in the Department of Anthropology at the University of Texas at Austin.